


Topic #51. Infant Part 4. Breastfeeding Jaundice and Breast Milk Jaundice
February 3, 2025

This objective of this post is to review the difference between breastfeeding jaundice and breast milk jaundice.
Breastfeeding Jaundice
It’s called breastfeeding jaundice but perhaps a better term would be - lack of breastfeeding jaundice.
Onset is in the first days of life
Cause is poor breast feeding with delayed pooping leading to increased enterohepatic circulation of unconjugated bilirubin
Clinically expect to see poor breastfeeding, excessive weight loss, a sleepy or fussy baby and decreased urine and stool output
Treatment
FEED THE BABY (While it would be easy to just formula feed, consider an approach where you don’t sabotage the breastfeeding by using a supplemental feeding plan, described below)
Fix or work on the breastfeeding problem
Monitor closely
Supplemental feeding plan
The goal of a supplemental feeding plan is to feed the baby but not break the breastfeeding. Here is the supplemental feeding plan we use at our hospital.
The baby should feed from the breast on feeding cues. Mother should pump after feeds (at least every three hours). Feed the baby expressed mother’s milk/donor milk/infant formula of the following volume via an alternative feeding method of mother’s choice.
0-24 hours, up to 10-15cc per feed every three hours
25-48 hours, up to 20 cc per feed every three hours
49 -72 hours, up to 30 cc per feed every three hours
Alternative feeding method per the mother’s choice: cup/syringe/finger feed/dropper/bottle (slow flow nipple, pace feed)
So let’s say the infant is 38 hours old. The baby would go to breast when showing feeding cues, the mother would pump every three hours (after feeds) and then the baby would be fed 20 cc of pumped or expressed breast milk plus donor milk (if available and mother is ok with that) or infant formula. The mother would pick what type of alternative feeding method to use.
Phototherapy
If the bilirubin level is high enough, the infant may need to be placed on phototherapy or “go under the lights”
Phototherapy works by the fact that the energy of the light converts the unconjugated (fat soluble) bilirubin to a different shape/configuration which is water soluble. This new form of bilirubin can be peed out in the urine.
Phototherapy
Blue-green light
Fluorescent tubes, tungsten halogen lamps, fiberoptic blanket
Exposure to infant’s maximum surface area
Baby should be in a bassinet, not an incubator
Fluorescent tubes are placed at a certain distance from the infant
The default in our hospital is two device phototherapy which means a neo blue bank above and a bili blanket under the infant. This is shown in the picture below.

When the baby comes out to breastfeed, while breastfeeding, the bili blanket goes on the baby’s back.

Breast Milk Jaundice
Breast milk jaundice is a benign unconjugated hyperbilirubinemia associated with breastfeeding.
Breast milk jaundice:
Is a common cause of prolonged jaundice in an otherwise healthy breastfed infant born at term
Presents in the 1st or 2nd week of life
Can persist for as long as 12 weeks before spontaneous resolution
Has been reported as affecting as many as one-third of exclusively breastfeeding infants
Presents as this clinical picture: the baby is thriving, eating well, with good weight gain and is peeing and pooping normally
What causes breast milk jaundice?
The exact cause of breast milk jaundice has not been determined. Some theories:
Beta glucuronyl transferase in the gut deconjugates the bilirubin which then gets sucked back into the blood stream
Epidermal growth factor in human milk
Something in breast milk that interferes with the conjugation step in the liver hepatocytes
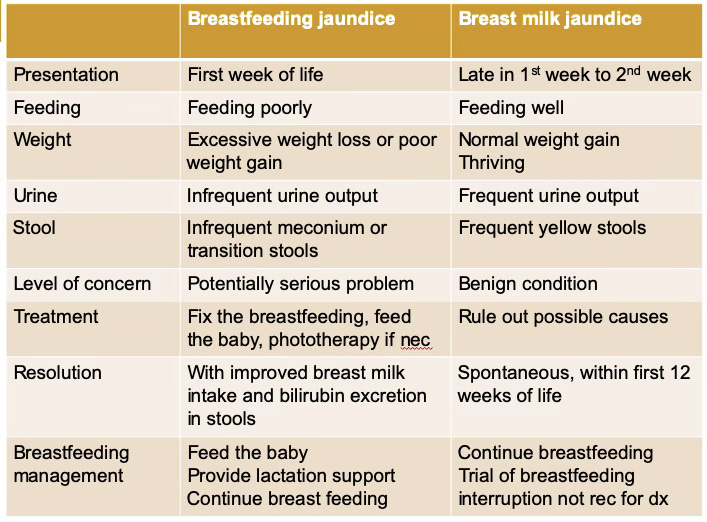
A table comparing the two
This table compares breastfeeding jaundice and breast milk jaundice.
References
Preer GL, Philipp BL. Understanding and managing breast milk jaundice. Arch Dis Child Fetal Neonatal Ed. 2011 Nov;96(6):F461-466
Tema #51. Ictericia de Lactancia y Ictericia de la Leche Materna
El objetivo de esta publicación es ayudarlo a comprender la diferencia entre dos afecciones, la ictericia de la lactancia materna y la ictericia de la leche materna.
Ictericia de lactancia materna
Esto se llama ictericia de lactancia, pero quizás un término mejor es “falta de ictericia de lactancia”.
El inicio es en los primeros días de vida.
Causa: lactancia materna deficiente, defecación tardía que conduce a un aumento de la circulación enterohepática de bilirrubina no conjugada
Clínicamente: pérdida de peso excesiva, lactancia deficiente, bebé somnoliento o irritable, disminución de la producción de orina y heces
Tratamiento:
ALIMENTAR AL BEBÉ (use un plan de alimentación suplementario, descrito a continuación)
Arreglar o trabajar en el problema de la lactancia
Monitorear de cerca
Un plan de alimentación suplementaria
El objetivo de un plan de alimentación suplementaria es alimentar al bebé pero no interrumpir la lactancia.
Este es el plan de alimentación suplementaria que utilizamos en nuestro hospital.
El bebé debe alimentarse del seno cuando se le indique. La madre debe extraer leche después de las tomas (al menos cada tres horas). Alimente al bebé con leche materna extraída/leche de donante/fórmula infantil del siguiente volumen a través de un método de alimentación alternativo elegido por la madre.
0-24 horas, hasta 10 cc por alimentación cada tres horas
25-48 horas, hasta 20 cc por toma cada tres horas
49 -72 horas, hasta 30 cc por toma cada tres horas
Método de alimentación alternativo según la elección de la madre: taza/jeringa/alimentación con el dedo/cuentagotas/biberón (tetina de flujo lento, alimentación a ritmo)
Es posible que el bebé deba recibir fototerapia o "ir bajo las luces"
La fototerapia funciona por el hecho de que la energía de la luz convierte la bilirrubina no conjugada (soluble en grasa) en una forma/configuración diferente que es soluble en agua. Esta nueva forma de bilirrubina se puede orinar en la orina.
Fototerapia
Luz azul-verde
Tubos fluorescentes, lámparas halógenas de tungsteno, manta de fibra.
Exposición al área de superficie máxima del bebé
El bebé debe estar en un moisés, no en una incubadora.
Los tubos fluorescentes se colocan a cierta distancia del bebé.
El valor predeterminado en nuestro hospital es la fototerapia de dos dispositivos, lo que significa un banco neo azul arriba y una manta de bili debajo.
Cuando el bebé sale a amamantar, durante la lactancia, la manta de bili va sobre la espalda del bebé.
Ictericia de la leche materna
Ictericia de la leche materna es una hiperbilirrubinemia no conjugada benigna asociada con la lactancia.
Una causa común de ictericia prolongada en un bebé amamantado por lo demás sano nacido a término
Se presenta en la 1ª o 2ª semana de vida.
Puede persistir hasta 12 semanas antes de la resolución espontánea
Se ha informado que afecta hasta a un tercio de los bebés que amamantan exclusivamente
Clínicamente el bebé está prosperando, comiendo bien, con un buen aumento de peso y está orinando y defecando normalmente.
La cause
No se ha determinado la causa exacta de la ictericia de la leche materna. Algunas teorías
La beta glucuronil transferasa en el intestino desconjuga la bilirrubina que luego es succionada nuevamente
Factor de crecimiento epidérmico en la leche humana
Algo en la leche materna que interfiere con el paso de conjugación en los hepatocitos del hígado
Referencias
Preer GL, Philipp BL. Understanding and managing breast milk jaundice. Arch Dis Child Fetal Neonatal Ed. 2011 Nov;96(6):F461-466