


Topic #56. Infant Part 9. Congenital Heart Disease
February 14, 2025

The topic of congenital heart disease can be confusing. Let’s try to break it down by looking at 5 topics:
Normal heart anatomy
Ductus arteriosus and patent ductus arteriosus
Congenital heart disease screen
Coarctation of the aorta
Cyanotic congenital heart disease
Normal heart anatomy
The four chambers of the heart are the right atrium, right ventricle, left atrium, and left ventricle. The atria (plural for atrium) receive blood (either from the body or from the lungs) and the ventricles pump the blood (either to the lungs or to the body). Arteries take blood away from the heart, veins bring blood to the heart. The heart contains four valves: tricuspid valve, pulmonic valve, mitral valve, and the aortic valve.
Think of the normal heart as having two sides. The right-side deals with deoxygenated (bluish) blood. The left side deals with oxygenated (red) blood. Two big veins, the inferior vena cave and the superior vena cava, collect blood from the body and bring that deoxygenated blood into the right atrium. From there the blood goes to the right ventricle which sends blood to the lungs via the pulmonary artery. In the lungs the blood is oxygenated again.
The oxygenated blood from the lungs travels via the pulmonary veins into the left atrium, then into the left ventricle, and then out to the body via the aorta.
Ductus arteriosus and patent ductus arteriosus
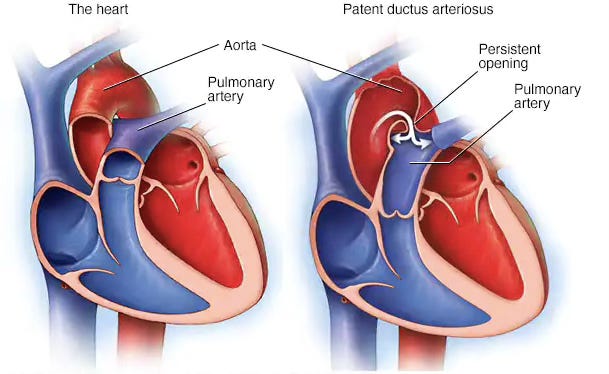
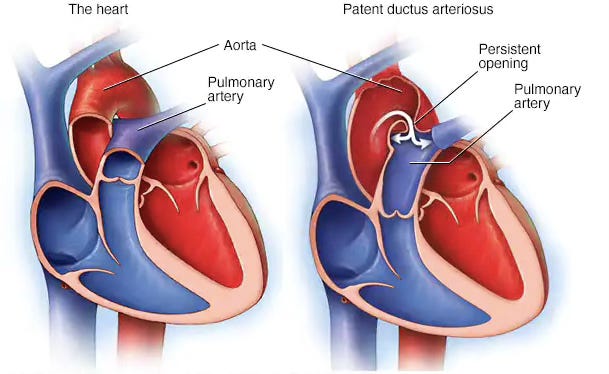
During fetal circulation, with the fetus is in utero developing and attached to the placenta, the mother (via the placenta) is taking care of oxygenating the fetus’ blood. Therefore, the fetus’ heart is set up to shunt blood AWAY from the infant’s lungs because there is no need for it to go to the lungs. The lungs in utero are not working as normal lungs would work. The shunting is done by a connection between the pulmonary artery and the aorta, called the ductus arteriosus. The pressure in the fetus’ lungs is high so the blood feels a block when it tries to go into the lungs and takes the easier route which is from the pulmonary artery to the aorta, bypassing the lungs.
One the infant is born, there is a shift to normal heart circulation. The infant takes a first breath and then continues to breath in oxygen and breath out carbon dioxide. Now getting blood into the lungs will oxygenate it and is necessary for the infant to survive. The patent or open ductus arteriosus normally closes within 1-2 days after birth. If it doesn’t close then the heart lesion is called a PDA or patent ductus arteriosus.
This is why the screen for congenital heart disease is done after 24 hours of life, to give the ductus arteriosus time to close. Then one can assess if the infant’s heart is set up properly.
Congenital heart disease screen
A standard of care on maternity units is to perform a heart disease screen once the infant is more than 24 hours of life. An oxygen saturation probe is placed on the infant’s right hand and right foot. To pass the screen, each reading must be over 94% and there must not be more than 3 units differing between the numbers.

Coarctation of the aorta
Remember that the blood in the left side of the heart is oxygenated. The left ventricle squeezes and send this rich, red blood out to the entire body via the aorta. Imagine the troubles if that aorta is constricted in any way and not all the rich, red blood can get out.
Think of it like a road block. Sometimes a road block is total – no cars are allowed. In the case of the road block police are present or a sign is present slowing traffic down, telling cars to stop or redirecting traffic away from the block.
But in the heart there is no policeman and the left ventricle keeps pumping and pumping trying to get the blood through the block. Eventually it is just too much and the heart can’t keep doing this and goes into failure. The patient is short of breath and breathing heavily. Depending where the block is will affect blood pressure reading. If the block is after where the arteries branch off, blood pressure in the upper arms will be sky high, blood pressure beyond the block, let’s say in the legs is thready or not palpable at all. The legs would feel cool to touch.
Cyanotic heart disease
For cyanotic congenital heart disease, use T is for Trouble and the Five Ts, to remember the names of the classic cyanotic congenital heart diseases.
The Five Ts
Truncus arteriosus
Transposition
Tricuspid atresia
Tetralogy of Fallot
Total anomalous pulmonary venous return (TAPVR)
Transposition of the great arteries is associated with severe cyanosis in the first hours after birth. The other “Ts” usually do not present with severe cyanosis.
Use the fingers on one hand to help remember the lesions. Hold up your hand:
1st finger – truncus arteriosus – in this lesion, one great vessel leaves the heart instead of two
2 fingers - hold up two fingers and cross them – transposition – the two main arteries leaving the heart are crossed

3 fingers - tri means three – tricuspid atresia – the tricuspid valve forms incorrectly
4 fingers – tetra means four – tetralogy of Fallot – this lesion has four things going on: pulmonic stenosis, right ventricular hypertrophy, overriding aorta and ventricular septal defect. No need to remember what the four things are, just remember tetra means four
5 fingers – what lesion has five words in it? – that would be total anomalous pulmonary venous return (TAPVR)
As Ina Garten would say, “How easy is that?”
Question 1.
A one-hour-old infant is noted to be blue in color. A nurse at first wonders if this is acrocyanosis but once the infant is in the nursery, on the warmer, cyanosis is noted in the lips, mucous membranes, and tip of the tongue. An oxygen saturation monitor on the infant’s right hand and right foot reads 85%. What is going on here?
A. Atrial septal defect
B. Ventricular septal defect
C. Patent ductus arteriosus
D. Transposition
The answer is D. This infant has central cyanosis. All of the answers refer to the heart so think about cyanotic heart disease. Remember T is for Trouble and the Five Ts. Only one of the Five Ts is in the answer – transposition - so that’s it. Remember if it starts with a T – it is a good bet it is a cyanotic heart lesion.
And remember transposition of the great arteries is associated with severe cyanosis in the first hours after birth so that fits. The other “Ts” usually do not present with severe cyanosis. So, this fits too.
Tema #56. Infantil Parte 9. Cardiopatías Congénitas
El tema de las cardiopatías congénitas puede resultar confuso. Intentemos desglosarlo analizando 5 temas:
Anatomía normal del corazón
Ductus arterioso y conducto arterioso permeable
Detección de enfermedades cardíacas congénitas
Coartación de la aorta
Cardiopatía congénita cianótica
Anatomía normal del corazón
Las cuatro cámaras del corazón son la aurícula derecha, el ventrículo derecho, la aurícula izquierda y el ventrículo izquierdo. Las aurículas (plural de aurícula) reciben sangre (ya sea del cuerpo o de los pulmones) y los ventrículos bombean la sangre (ya sea a los pulmones o al cuerpo). Las arterias toman sangre del corazón, las venas llevan sangre al corazón. El corazón contiene cuatro válvulas: válvula tricúspide, válvula pulmonar, válvula mitral y válvula aórtica.
Piense en el corazón normal como si tuviera dos lados. El lado derecho se ocupa de la sangre desoxigenada (azulada). El lado izquierdo se ocupa de la sangre oxigenada (roja). Dos grandes venas (la vena cava inferior y la vena cava superior) recogen sangre del cuerpo y la llevan desoxigenada a la aurícula derecha. Desde allí la sangre pasa al ventrículo derecho, que envía sangre a los pulmones a través de la arteria pulmonar. En los pulmones la sangre se vuelve a oxigenar.
La sangre oxigenada de los pulmones viaja a través de las venas pulmonares hacia la aurícula izquierda, luego hacia el ventrículo izquierdo y luego hacia el cuerpo a través de la aorta.
Ductus arterioso y conducto arterioso permeable
Durante la circulación fetal, con el feto en desarrollo en el útero y adherido a la placenta, la madre (a través de la placenta) se encarga de oxigenar la sangre del feto. Por lo tanto, el corazón del feto está configurado para desviar la sangre ALEJADA de los pulmones del bebé porque no es necesario que vaya a los pulmones. Los pulmones en el útero no funcionan como lo harían los pulmones normales. La derivación se realiza mediante una conexión entre la arteria pulmonar y la aorta, llamada conducto arterioso. La presión en los pulmones del feto es alta, por lo que la sangre se siente bloqueada cuando intenta llegar a los pulmones y toma la ruta más fácil que va de la arteria pulmonar a la aorta, sin pasar por los pulmones.
Una vez que nace el bebé, se produce un cambio hacia la circulación normal del corazón. El bebé respira por primera vez y luego continúa inhalando oxígeno y exhalando dióxido de carbono. Ahora, llevar sangre a los pulmones los oxigenará y es necesario para que el bebé sobreviva. El conducto arterioso permeable o abierto normalmente se cierra entre 1 y 2 días después del nacimiento. Si no se cierra, la lesión cardíaca se denomina CAP o conducto arterioso persistente.
Es por eso que la prueba de detección de cardiopatías congénitas se realiza después de las 24 horas de vida, para darle tiempo al conducto arterioso para que se cierre. Entonces se puede evaluar si el corazón del bebé está configurado correctamente.
Prueba de detección de cardiopatías congénitas
Un estándar de atención en las unidades de maternidad es realizar una prueba de detección de cardiopatías una vez que el bebé tiene más de 24 horas de vida. Se coloca una sonda de saturación de oxígeno en la mano y el pie derechos del bebé. Para pasar la prueba, cada lectura debe ser superior al 94% y no debe haber más de 3 unidades de diferencia entre los números.
Coartación de la aorta
Recuerde que la sangre en el lado izquierdo del corazón está oxigenada. El ventrículo izquierdo se contrae y envía esta sangre rica y roja a todo el cuerpo a través de la aorta. Imagine los problemas si esa aorta se contrae de alguna manera y no puede salir toda la sangre rica y roja.
Piense en ello como un bloqueo de carretera. A veces, un bloqueo de carretera es total: no se permiten automóviles. En el caso del bloqueo de carretera, la policía está presente o hay una señal que reduce la velocidad del tráfico, indicando a los automóviles que se detengan o redirigiendo el tráfico fuera del bloqueo.
Pero en el corazón no hay policía y el ventrículo izquierdo sigue bombeando y bombeando tratando de que la sangre atraviese el bloqueo. Al final, es demasiado y el corazón no puede seguir haciéndolo y entra en insuficiencia. El paciente tiene dificultad para respirar y respira con dificultad. Dependiendo de dónde se encuentre el bloqueo, afectará la lectura de la presión arterial. Si el bloqueo está después de donde se ramifican las arterias, la presión arterial en la parte superior de los brazos será altísima, la presión arterial más allá del bloqueo, digamos en las piernas, será filigrana o no se palpará en absoluto. Las piernas se sentirán frías al tacto.
Enfermedad cardíaca cianótica
Para la enfermedad cardíaca congénita cianótica, utilice T de Trouble y las cinco T para recordar los nombres de las enfermedades cardíacas congénitas cianóticas clásicas.
Las cinco T
Tronco arterioso
Transposición de las grandes arterias
Atresia tricúspide
Tetralogía de Fallot
Retorno venoso pulmonar anómalo total (TAPVR)
La transposición de las grandes arterias se asocia con cianosis grave en las primeras horas después del nacimiento. Las otras "T" generalmente no presentan cianosis grave.
Use los dedos de una mano para ayudar a recordar las lesiones. Levante la mano
1.er dedo: tronco arterioso; en esta lesión, un gran vaso sale del corazón en lugar de dos
2 dedos: levante dos dedos y crúcelos: transposición; las dos arterias principales que salen del corazón están cruzadas
3 dedos: tri significa tres; atresia tricúspide; la válvula tricúspide se forma incorrecta
4 dedos: tetra significa cuatro; tetralogía de Fallot; esta lesión tiene cuatro cosas en juego: estenosis pulmonar, hipertrofia ventricular derecha, cabalgamiento de la aorta y defecto del tabique ventricular. No es necesario recordar cuáles son las cuatro cosas, solo recuerde que tetra significa cuatro
5 dedos: ¿qué lesión tiene cinco palabras? – eso sería retorno venoso pulmonar anómalo total (TAPVR)
Como diría Ina Garten, "¿Qué tan fácil es eso?"
Pregunta 1.
Se observa que un bebé de una hora de nacido tiene un color azul. Una enfermera al principio se pregunta si esto es acrocianosis, pero una vez que el bebé está en la guardería, en la cuna, se nota cianosis en los labios, las membranas mucosas y la punta de la lengua. Un monitor de saturación de oxígeno en la mano derecha y el pie derecho del bebé indica 85%. ¿Qué está pasando aquí?
A. Defecto del tabique auricular
B. Defecto del tabique ventricular
C. Ducto arterioso persistente
D. Transposición de las grandes arterias
Respuesta. D) Transposición de las grandes arterias
Este bebé tiene cianosis central. Todas las respuestas se refieren al corazón, así que piense en la enfermedad cardíaca cianótica. Recuerde las cinco T. Solo una de las cinco T está en la respuesta: transposición, así que eso es todo. Recuerde que si comienza con T, es muy probable que se trate de una lesión cardíaca cianótica.
Y recuerde que la transposición de las grandes arterias se asocia con cianosis grave en las primeras horas después del nacimiento, así que esto encaja. Las otras "T" generalmente no se presentan con cianosis grave. Por lo tanto, esto también encaja.
I enjoyed reading this, it's very interesting and useful. When I was pregnant with my third child, almost 18 years ago, he was diagnosed with a heart defect which was confirmed as coarctation of the aorta when he was born. He was very poorly and he died during surgery but hearts have fascinated me ever since.